|
|
| Do you believe in magic? |
|
|
SHELDON H. PRESKORN, MD
|
|
Journal of Practical Psychiatry and Behavioral Health, March 1997, 99-103
|
We are all susceptible to wanting to believe in magic, particularly when circumstances seem hopeless without it. Sometimes, we are aware that we are counting on a magical solution. At other times, we are not--this can be the case when the clinician succumbs to the use of "psychopharmacological magic."
Magic is defined in Webster's dictionary as the "art that purports to control events in nature through the use of charms, spells, rituals or potions." In clinical psychopharmacology, the parallel to the sorcerer's potions are the complicated admixtures of different mood stabilizers, antipsychotics, antidepressants, and anxiolytics that clinicians sometimes resort to when treating patients. These "cocktails" are generally based on no systematic data of safety or efficacy but instead arise out of the clinician's belief or hope that a medication regimen must exist that will produce the desired clinical response in the patient and that the best way to find it is simply to add medications until the desired response occurs. Unfortunately, this practice can lead to convoluted cases of polypsychopharmacy with adverse consequences. We will explore this subject in this column and use a case to illustrate some of the major points.
THE RATIONALE BEHIND POLYPHARMACY
Polypharmacy is widespread. Based on the results of recent surveys, 30%--80% of patients who are taking an antidepressant are also taking at least two other drugs.1 A sizable percentage of patients are thus being treated with combinations of medications, often without much in the way of rigorous research to support the safety and efficacy of specific combinations.
There are many forces fueling this practice. I will address this issue at greater length in another column but one factor deserves comment here: an apparent growing belief in the almost mystical powers of pharmacology. That belief appears to have largely replaced the earlier belief in the mystical powers of psychotherapy. I began my psychiatric career in an era dominated by a pervasive belief in the abilities of insight-oriented psychotherapy to cure every type of psychiatric problem. In that era, the use of medication was generally viewed as either a sign of failure or a lack of faith.
There is now almost the same belief that psychopharmacology can cure any psychiatric problem. That belief has been spurred by the undeniable advances that have been made in clinical psychopharmacology over the last one to two decades. There are, however, major limitations to this approach. First, the pathophysiology of psychiatric disorders remains largely unknown. Second, medications are, after all, simple molecules with limited effects. Third, psychiatric medications are designed to affect the brain and thus their adverse effects can mimic psychiatric symptoms. If the clinician does not keep that possibility in mind, he or she may respond to a medication's adverse effect as if it were a worsening of the underlying illness and either increase the dose of the offending medication or add other medications. In this column, I focus on just such a case.
With further research, we will likely improve our ability to somatically treat and in some instances even prevent psychiatric illnesses. Future practitioners may look back on our attempts to treat some of these illnesses with existing medications as well intentioned but naive. In the future, we will also be better able to divide psychiatric disorders into those that are predominantly due to "hardware" problems and those due to "software" problems. The latter will likely be found to be better treated with "software" rather than "hardware" interventions. Obviously, the clinician today has to rely on the tools currently available but must take a disciplined approach to their use and be mindful of the possibility that the optimal tool may not exist. To do this requires a balancing act in the sense that the clinician wants to hold out hope to the patient but at the same time cannot allow hope to override careful judgment. This is particularly important when the temptation arises to resort to complicated polypsychopharmacy as is illustrated in the following case.
CASE EXAMPLE
A 17-year-old female became distressed after breaking up with her first boyfriend. She was taken by her mother to a senior psychiatrist in another community after she made superficial cuts on her arm. Her past psychiatric history was unremarkable. She had been an A and B student in school, but her grades had recently declined following the breakup. She had no truancy or disciplinary problems at school but had been more irritable and sullen at home. After 8 months of care she was on the following regimen:
| Lithium | 1200 mg/day | | Carbamazepine | 500 mg/day | | Valproate | 1750 mg/day | | Fluoxetine | 40 mg/day | | Risperidone | 3 mg/day | | Benztropine | 1 mg/day | | Ranitidine | 300 mg/day |
She came to our community for the summer to stay with her father, who requested a second opinion. The interview was difficult because the patient would fall asleep unless she was actively engaged and prompted by the interviewer. While the father was receptive to the recommendation to attempt to simplify the current regimen, her mother was convinced that her daughter would significantly deteriorate if any of the medications were stopped or even reduced.
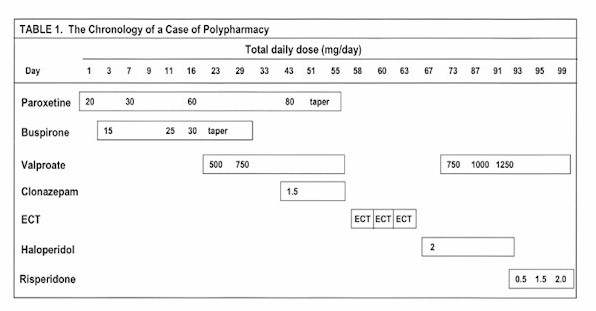
In our evaluation, we found no medical problems. Plasma drug levels of the first five drugs listed above were consistent with the prescribed doses. The longitudinal course of her prior treatment was plotted based on her medical records (Table 1). Only the first 3 months are shown for brevity's sake, since they sufficiently illustrate the major point that will be discussed in this column.
DISCUSSION
Treatment with SSRIs
At her first visit, this patient was begun on the selective serotonin reuptake inhibitor (SSRI) paroxetine. In the era in which I began my psychiatric career, she would undoubtedly have been treated solely with psychotherapy. In this era of managed care, it has become the spirit of the time to give the appearance of treating efficiently by prescribing a medication at the first visit. That may well speed response in some patients but may also result in the unnecessary use of medication in patients who have a more transient disturbance. If this patient's symptoms had persisted over time, even for the interval between the first two visits, then the potential need for medication would have been better supported.
Nevertheless, the safety and tolerability profile of SSRIs such as paroxetine is such that a significant percentage of clinicians, perhaps even the majority, might agree with the decision to initiate an empirical trial in this case at the first visit. However, an empirical trial requires discipline and patience. Neither were obvious in the management of this case.
SSRIs as a class have a flat dose-response curve, meaning that, on average, there is no advantage to raising the dose above the usually effective dose in most patients. The flat dose-response curve is consistent with the fact that these drugs appear to have a single mechanism of action mediating their antidepressant efficacy -- serotonin uptake inhibition. It is also consistent with in vivo human studies that have used the effect of the SSRIs on platelet serotonin uptake as a surrogate marker for what is occurring in the brain. All of the SSRIs produce the majority of their serotonin uptake inhibition at their usually effective dose. Higher doses, on average, produce only modest additional increases in such inhibition.
As discussed in my November 1996 column, interindividual differences in clearance and pharmacodynamic sensitivity are such that there are undoubtedly some patients who would respond better to a dose that is either lower or higher than the usually effective dose. Nevertheless, it is incumbent on the clinician to document the need for a dose other than the usually effective dose. That could be done by measuring the plasma drug level and demonstrating that the patient clears the drug in question either considerably faster or slower than the usual patient so that the dose the patient is receiving is functionally lower or higher respectively than the usually effective dose in the usual patient. That approach is rarely followed in clinical practice with SSRIs even though it could be. Another approach is to document that the patient needs a different dose based on careful clinical assessment of response. For example, a lower dose could be supported by the documentation that the patient has more dose-dependent adverse effects (either in terms of number or severity) than would usually be expected of the usually effective dose. Conversely, a higher dose could be supported by the documentation that the patient failed to respond to an adequate trial of the usually effective dose. For SSRIs, an adequate trial would take at least 4 weeks on the usually effective dose and perhaps a comparable interval on each higher dose.
This patient did not receive an adequate trial of the usually effective dose of paroxetine, which is 20 mg/day. She was on this dose only 6 days before it was escalated to 30 mg/day. Within 2 weeks of starting this drug, she was on 60 mg/day, which is above the maximum recommended dose in adults. This patient was kept on 60 mg/day for 3 weeks and then the dose was escalated to 80 mg/day.
There are no systematic data on what should be the recommended maximum daily dose for adolescents, but it would seem prudent to use caution when exceeding the dose for adults, even though adolescents conceivably may clear the drug faster than adults and thus could need higher doses. Again, either careful clinical documentation and/or the use of therapeutic drug monitoring to support such doses would be prudent. Given the pharmacology of SSRIs, the rationale behind the use of doses well above the usually recommended maximum would seem to be based more on a belief in magic than on scientific principles.
Of importance, SSRIs produce a number of dose-dependent adverse effects that could mimic worsening of the underlying illness. These include agitation, restlessness, anorexia, insomnia, and daytime fatigue. This patient reported these symptoms. The question is whether they occurred despite the medication or because of the medication. Consistent with the almost universal bias that failure to optimally respond must mean the dose is too low, the reports of these symptoms in this case led to dose escalation followed by further deterioration in an apparent vicious cycle.
Augmentation with Buspirone
Interpretation of this patient's trial of paroxetine is further complicated by the rapid addition and subsequent periodic dose escalation of buspirone, another serotonin active medication. The addition of this drug raises the possibility of clinically significant pharmacokinetic and pharmacodynamic drug-drug interactions. While the pharmacodynamic interactions are complex and a full discussion is beyond the scope of this column, a brief discussion follows to emphasize what the clinician needs to keep in mind when using polypharmacy.
Paroxetine and buspirone act on different but related central serotonin (5-HT) mechanisms, paroxetine as an inhibitor of the serotonin uptake pump and buspirone as a partial agonist of the 5-HT1a receptor. This receptor presynaptically regulates serotonin cell firing and postsynaptically mediates effects on serotonin in specific terminal fields of its neural projections. Blockade of the presynaptic 5-HT1a receptor can produce a loss of the feedback mechanism, which prevents overactivity of the serotonin system.
The central 5-HT effects of buspirone are complex.2, 3 Buspirone is a partial 5-HT1a agonist and hence its net effect is a function of the concentration of 5-HT at the receptor. If the concentration of 5-HT is low, then buspirone will act as an agonist. If the concentration of 5-HT is high, then buspirone, being a partial agonist, will antagonize the effect of excessive 5-HT. In addition, buspirone acts at postsynaptic as well as presynaptic 5-HT1a receptors, which mediate different physiological mechanisms in the brain.
The pharmacology in this case is made more complicated by the fact that buspirone is converted to a centrally active metabolite, 1-phenyl-piperazine (1-PP).4 This metabolite, like buspirone, acts at the 5-HT1a receptor5 but is even more potent as an alpha-2 adrenergic receptor blocker acting at somatodendritic and terminal alpha-2 adrenergic autoreceptors and postsynaptic alpha-2 adrenoreceptors.6,7 Thus, to the mix operating in this case, this metabolite adds direct central norepinephrine effects similar to those of yohimbine and opposite of those of clonidine.8 Moreover,1-PP has been shown to be able to both potentiate and antagonize the effects of its parent drug, buspirone.5,9,10
This metabolite is likely to have played more of a role in this case than if buspirone had been used alone because its levels were likely elevated by coadministration with paroxetine. 1-PP is likely to be principally metabolized by the cytochrome P450 (CYP) enzyme 2D6 given its structural similarity to meta-chlorophenylpiperazine, a known CYP 2D6 substrate. Paroxetine at 20 mg/day produces 85% inhibition of CYP 2D6.1 At the doses used in this case, CYP 2D6 was most likely fully inhibited, leading to much higher than usual 1-PP accumulation.
Based on the fact that buspirone affects 5-HT mechanisms and hence could alter the response to SSRIs, some clinical researchers have added buspirone to the treatment regimen of patients who have not benefited from treatment with an SSRI alone.11-14 Like all augmentation strategies, the goal of using buspirone in combination with an SSRI is to produce a drug-drug interaction that will be therapeutic for the patient. The clinician needs to be aware that pharmacologically the net result is to increase or decrease the effect of the first drug by altering its pharmacodynamics or pharmacokinetics. The net result may be advantageous or disadvantageous depending on what change is affected and to what extent.
Case reports of such augmentation strategies often spur their use. However, the clinician needs to be aware of their limitations. First, they are often based on quite small numbers of patients. Second, they are uncontrolled so that it is difficult to assess with confidence either the tolerability of efficacy of the combination. Third, the reports generally focus on efficacy, often with hardly a mention of adverse consequences. There have, however, been reports that the addition of buspirone to an SSRI might have consequences ranging from euphoria to mania to seizures.13,15,16
In this case, the patient almost undoubtedly had substantial serotonin uptake inhibition to which were added the effects of buspirone and 1-PP on both 5-HT1a and alpha-2 adrenergic receptors. Such a combination of effects could potentially cause a partial central serotonin syndrome, which can present as either delirium or mania.17 Consistent with this possibility and with two previous case reports,13,16 this patient developed signs of mania on day 23 of treatment.
Further Treatment Adjustments
On day 23, the decision was made to discontinue buspirone and add valproate for the emerging mania. This series of events is consistent with the fact that adverse effects due to psychotropic medications or combinations of medications can mimic psychiatric symptomatology and can result in more medications being added rather than in the treatment regimen being simplified. This explanation, while not verified in this case, is certainly plausible given the facts.
On day 43, paroxetine was increased to 80 mg/day, which is four times the usually effective dose and well above the maximum recommended dose for adults. As mentioned above, the clinician could have used therapeutic drug monitoring to document the need for such a dose to achieve the plasma levels of paroxetine that normally occur on the usual effective dose of 20 mg/day in "usual" patients. However, such monitoring was not done in this case.
On day 43, clonazepam was also added because of increasing agitation, which is a dose-dependent adverse effect of SSRIs. Again, the clinician may have been adding a medication to treat an adverse effect resulting from excessive serotonin uptake inhibition. Consistent with that explanation, the agitation worsened after the paroxetine dose was increased, causing the clinician to "taper" the patient from 80 mg/day to 0 mg/day over 4 days. Withdrawal has been reported following the abrupt discontinuation of SSRIs. The relative risk and the severity of such withdrawal is a function of the daily dose and the half-life of the SSRI. Withdrawal can cause a number of symptoms that can mimic a worsening of the patient's psychiatric status, including agitation, irritability, aggression, tremulousness, sleep disturbance, nightmares, difficulties concentrating, "racing thoughts," and confusion.
This patient developed most of these symptoms during the "taper," which were interpreted as signs that the patient was becoming more "manic." For that reason, valproate and clonazepam were abruptly discontinued on day 55 and the patient was given three electroconvulsive treatments (ECT). The effects of these treatments were thus superimposed on a state of SSRI withdrawal, which typically takes at least 1-2 weeks to resolve on its own. The ECT treatments were discontinued because the patient's psychiatric state deteriorated further. She was then started on an antipsychotic for a suspected emerging psychosis. Subsequently, valproate and clonazepam were reinstituted and haloperidol was switched to risperidone. The patient eventually ended up on the regimen outlined at the beginning of this column.
Our Evaluation
When faced with this case, we were uncertain which of the medications, if any, were in fact needed. Conceivably, all of them were needed exactly as prescribed -- but it was also conceivable that none of them were needed. In such instances, we take the reverse approach to what we prefer to do at the beginning. Whenever possible, we prefer to initiate treatment with adequate monotherapy trials to determine what effect a specific medication and ideally a specific mechanism of action will produce in the patient: beneficial response, an adverse response, or no effect. Since we could not do that in this case, we did the reverse: a slow taper of one medication at a time to assess what effect it was producing. The only exception to this gradual approach is when the clinical status of the patient demands that a more aggressive approach be taken. After 3 months, this patient was on lithium 900 mg/day and fluoxetine 20 mg/day with the only apparent consequence being an appreciable improvement in her functional status.
Since many psychiatric illnesses are cyclic and since this patient could be at risk for relapse for many months after a medication is discontinued, we still must be cautious in our conclusions and our follow-up. We would recommend maintaining the patient on this regimen for 3 months to obtain a new baseline. If no return of symptomatology occurs, we would continue a quite gradual taper of one of these two remaining medications. The goal is to treat the patient with the minimum number of medications necessary to achieve maximum functional status.
CONCLUSION
This case illustrates the complex considerations that must be kept in mind when resorting to polypsychopharmacy. It also illustrates the long commitment that such a treatment strategy requires. This is particularly true in an era in which some experts are recommending indefinite treatment with antidepressants on the basis of a small number of studies done in populations selected for a high risk of having recurrent episodes.
We recommend that clinicians be aware of the following considerations (in addition to those already enumerated above) when embarking on polypsychopharmacy:
- the potential for drugs to interact pharmacodynamically and/or pharmacokinetically to alter the expected effect or response
- the need to give disciplined trials of medications, ideally in isolation, before increasing the dose too quickly or too much or before adding other agents
- the need to consider that deterioration may be because of the drug therapy rather than in spite of it
- the need to realize that stopping medication is doing something as opposed to thinking that one is only doing something when one is adding medications
- the need to stop psychiatric medications properly, which often requires a gradual taper; otherwise withdrawal effects can mimic worsening of the underlying illness.
Without taking these factors into account, "psychopharmacologic magic" may turn out to be a curse rather than a blessing. In the end, blind faith in any treatment modality, whether psychotherapy or psychopharmacology, does not serve either the patient or the physician well.
References
- Preskorn SH, Clinical Pharmacology of Selective Serotonin Reuptake Inhibitors. Caddo, Okla: Professional Communications, Inc; 1996
- Sharp T., McQuade R., Bramwell S., Hjorth S, Effect of acute and repeated administration of 5-HT1A receptor agonists on 5-HT release in rat brain in vivo. Naunhyn Schmiedebergs Arch Pharmacol. 348(4):339-46;1993
- Van den Hooff P., Galvan M, Actions of 5-hydroxytryptamine and 5-HT1A receptor ligands on rat dorso-lateral septal neurons in vitro. Br J Pharmacol. 106(4):893-9;1992
- Grasby P., Sharp T., Moorman J., Grahame-Smith D, Comparison of the effect of buspirone and 1-(2-pyrimidinyl)piperazine on cerebral glucose utilization in the rat. Eur J Pharmacol. 230(1):41-6;1993
- Manahan-Vaughan D., Anwyl R., Rowan MJ, The azapirone metabolite 1-(2-pyrimidinyl) piperazine depresses excitatory synaptic transmission in the hippocampus of the alert rat via 5-HT1A receptors. Eur J Pharmacol. 294(2-3):617-24;1995
- Blier P., Curet O., Chaput Y., de-Montigny C, Tandospirone and its metabolite, 1-(2-pyrimidinyl) piperazine-II. Effects of acute administration of 1-PP and long-term administration of tandospirone on noradrenergic neurotransmission. Neuropharmacology. 39(7):691-701;1991
- Done CJ., Sharp T, Biochemical evidence for the regulation of central noradrenergic activity by 5-HT1A and 5-HT2 receptors: microdialysis studies in the awake and anaesthetized rat. Neuropharmacology. 33(3-4):411-21;1994
- Cao BJ., Li,WP, Antagonism of clonidine antinociception by buspirone and 1-(2-pyrimidinyl) piperazine. Eur J Pharmacol. 259(1):75-8;1994
- Martin P, 1-(2-pyrimidinyl) piperazine may alter the effects of the 5-HT1a agonist in the learned helplessness paradigm in rats. Psychopharmacology-Berl. 104(2):275-8;1991
- Przegalinski E., Tatarczynska E., Chojnacka-Wojcik E, Antidepressant-like activity of ipsapirone, buspirone and gepirone in the forced swimming test in rats pretreated with proadifen. Journal of Psychopharmacology. 4(4):204-9;1990
- Bakish D, Fluoxetine potentiation by buspirone: Three case histories. Can J Psychiatry. 36(10):749-50;1991
- Jacobsen FM, Possible augmentation of antidepressant response by buspirone. J Clin Psychiatry. 52(5):217-20;1991
- Robillard M., Lieff S, Augmentation of antidepressant therapy by buspirone: Three geriatric case histories. Can J Psychiatry. 40(10):639-40;1995
- Joffe RT, Schuller DR, An open study of buspirone augmentation of serotonin reuptake inhibitors in refractory depression. J Clin Psychiatry. 54(7):269-71;1993
- Grady TA, Pigott TA, L’Heureux F, Murphy DL, Seizure associated with fluoxetine and adjuvant buspirone therapy. J Clin Psychopharmacol. 12(1):70-1;1992
- Lebert F., Pasquier F., Goudemand M., Petit H, Euphoria with buspirone after fluoxetine treatment. Am J Psychiatry. 150(1):167;1993
- Sternbach H, The serotonin syndrome. Am J Psychiatry. 1991;148:705-713
|